doing anything, said Albert Einstein.
My name is Kadiyali Srivatsa. I brought tears of happiness to the eyes of 1000s of adults and children who suffered, until one cold winter day in December 1989.
A healthy boy aged 14 years walked into A&E in a hospital and died holding my hand that very evening.
WHY?
We scientists were so preoccupied with whether or not we could, that we did not stop to consider if we should. It is ironic that a science fiction film, Jurassic Park, aptly describes the medical crisis we face today. I am not talking about saving modern medicine, but about saving the lives of people like you. We are now confronting a mortal enemy that surpasses our own intelligence.
A tiny microorganism has indeed brought us to our knees. It has learned from us, adapted to us, and now exploits our genetic vulnerabilities with lethal precision. Sadly, those who dare to speak up are ridiculed, ignored, dismissed, and often ostracised by members of our own profession.
Yet the death toll mounts, while our greed, addiction toward, over enthusiastic urge to encourage consultation, perform tests, procedures, hospitalisation and antibiotic abuse escalates at alarming rates.
Pharmaceuticals, medical device manufacturers, government, and even some doctors ignore this Elephant in the room.
By not safeguarding the miracle drug as custodians, we have allowed antibiotics to be used to fatten chickens, treat animals, and encourage nurses with no formal medical training to utilise our skills, diagnose illnesses, prescribe drugs, and sell antibiotics without prescriptions. We have now lost the only drug that helped us fight infections, learn more about our bodies, make medical advances possible, perform surgical procedures, transplants, IVF, and save millions of lives. I sincerely hope we will change this destructive pattern of consultation and illness management.
In 1996, I published an article in the British Medical Journal to remind my colleagues that “The duty of a doctor is to listen to the story of a person”. My mission is to help encourage members of our profession to share knowledge, innovate, and develop products and methods to fight infection. Using advances in communication technology, I hope to provide basic healthcare to fellow humans, reduce healthcare costs, and decrease cross-infections that cause pain and suffering worldwide.
We must stop greedy entrepreneurs from commercialising our service to humanity.
Before I start rattling on about Our Ancestors, teachers, or our contribution to protecting humanity, Innovations, and fighting institutions, hospitals, and politicians for offering Sub-Standard care to fellow humans.
I beg members of my profession to shun their Ego, Share Knowledge, communicate, Communicate And Join Hands with us and help us stop this Elephant, In The Room, that is now,
Threatening our Profession and Our Very Existence.
#PremaKiosk. #DrMayaAI, #DigitalHealthIndia, #HealthcareInnovation, #CommunityHealthcare, #FutureOfHealthcare,
#PreventiveHealthcare, #AIinHealthcare, #SmartHealthcare, #HealthTechIndia, #InfectionPrevention, #PandemicPreparedness, #AntimicrobialResistance, #PublicHealthInnovation, #EarlyDetection, #HealthSecurity,, #DiseasePrevention, #OutbreakPrevention, #HealthcareSafety,#ProtectYourFamily, #HealthForAll #DignityInHealthcare, #FamilyFirstHealth, #HealthyCommunities, #ApartmentLivingIndia, #CommunitySafety, #SmartSociety, #SocialInnovation, #PurposeDrivenBusiness, #HealthcareStartup, #SocialEnterprise, #ArtificialIntelligence, #DigitalTransformation, #FutureTechnology, #TechForHumanity, #AI, #AIinHealthcare, #DrMayaAI, #DrMayaGPT, #Drkadiyalisrivatsa, #MayaMeditation, #AMR, #Antibiotics #doctors, #Doctor, #MayaAI #NewIndiaHealth,

 4 mins
4 mins 45 mins
45 mins Apr 10 202634 mins
Apr 10 202634 mins 26 mins
26 mins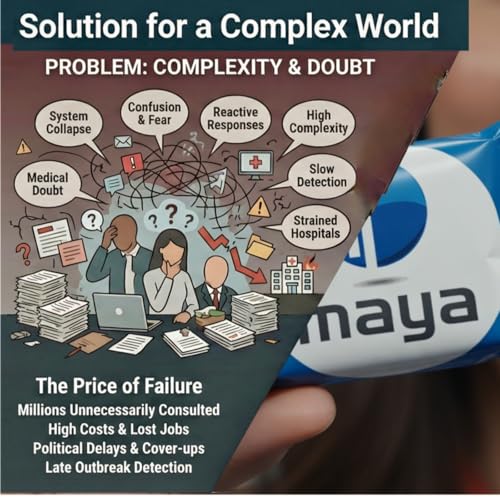 26 mins
26 mins 38 mins
38 mins 25 mins
25 mins 21 mins
21 mins